
Published on June 3, 2026
Summer heat can be dangerous, especially for children and older adults. Dr. Solomon Behar, a pediatric emergency medicine physician at Miller Children’s & Women’s Hospital, explains the warning signs of heat-related illness, when it becomes life-threatening, and how families can stay safe.
Frequently Asked Questions About Heat-Related Illness
Q: Summer is here and with it is heat related illness. How seriously should physicians take this?
A: As someone who grew up in the heat of the Las Vegas desert, I have seen the effects of too much heat firsthand. Heat has the potential to do great harm. Although heat-related illness sits on a spectrum, once a patient progresses to the dreaded heat stroke, where one loses their ability to control their core temperature, you’re dealing with a high-mortality, time-sensitive emergency. Even with treatment, outcomes depend on how quickly you can recognize it and lower the core temperature.
What makes it challenging is that early presentations are often nonspecific, including fatigue, dizziness, mild confusion, and these can be mistaken for dehydration, infection, or general deconditioning. If you’re not considering heat exposure related illness, it’s easy to miss.
Q: Who is most at risk for heat-related illness?
A: The extremes of age are at particular risk. Infants and young children have immature thermoregulation and rely on caregivers to control their environment, while older adults often have a blunted thirst response and may be on medications that impair fluid balance or heat dissipation.
Q: Heat stroke related deaths are projected to increase by nearly 2.5 times by 2050. How can physicians prepare for this?
A: Preparation is largely about recognizing heat related illness in the first place and then being ready to act quickly. Emergency Departments and inpatient care teams should be aligned on protocols so that once heat stroke is suspected, there’s no hesitation in initiating treatment and having the tools available for rapid cooling.
Q: I understand that heat stroke can present in a similar way to sepsis, meningitis, encephalitis, etc. How can physicians quickly differentiate between these and what is the best approach for treatment?
A: The most useful differentiator early on is clinical historical context. A history of recent heat exposure, exertion, or limited access to cooling or hydration should raise immediate concern for a heat-related cause of symptoms, even in the absence of a clear timeline. Priority should be given to early recognition and immediate initiation of active cooling, while simultaneously evaluating for infectious or neurologic causes.
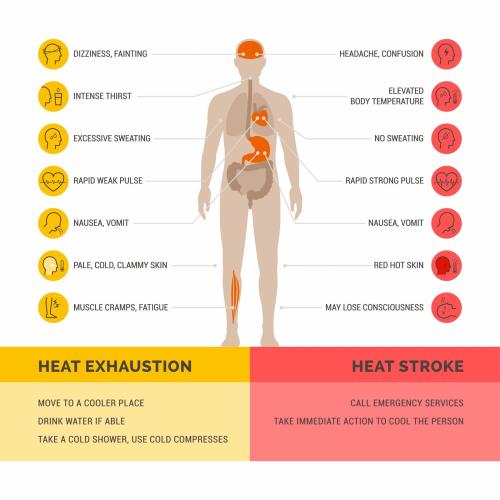
Q: How does heat stroke differ from heat exhaustion, and how should physicians approach each?
A: Heat exhaustion and heat stroke represent progressive stages along the spectrum of heat-related illness, distinguished primarily by the presence of thermoregulatory failure and neurologic dysfunction.
In heat exhaustion, the less severe of the two conditions, patients typically present with dehydration and intact thermoregulation. Clinical features include heavy sweating, fatigue, dizziness, nausea, and weakness. Core temperature may be elevated, but central nervous system function is preserved. Support includes removal from the heat, fluid repletion, and external cooling, with close reassessment to ensure symptoms resolve.
Heat stroke, by contrast, is defined by core temperature elevation and central nervous system dysfunction, including confusion, agitation, or decreased level of consciousness. At this stage, thermoregulation has failed, and there is risk of multisystem injury, including hepatic, renal, and neurologic damage.
Heat exhaustion requires monitoring and supportive care, whereas heat stroke is a time-sensitive emergency where the priority is rapid reduction of core temperature through active cooling, alongside standard resuscitative measures.
The line between exhaustion and stroke can be blurry, and progression between the two can occur, so early recognition and intervention in heat exhaustion is critical to preventing escalation to heat stroke.
Q: What is the first step a physician should take if they suspect a patient is experiencing heat stroke?
A: In heat stroke, outcomes are closely tied to how long the body stays overheated. So, the first step is to get the patient out of the heat, remove excess clothing, and start active cooling as aggressively as you can. Everything else, like giving cooled IV fluids, can happen alongside that.
Q: Patients may underestimate the impact heat can have on the body. What do you suggest physicians do to improve understanding and keep patients safe in the hotter months?
A: When thinking about heat, people tend to view it as uncomfortable rather than it being dangerous. To help keep patients safe, I suggest physicians advise that:
- Heat related illness can happen faster than people expect, especially in humidity.
- Feeling dizzy, nauseated, or confused is a warning sign.
- Drinking water helps for hydration, but you also need breaks in the shade and ways to cool down (think cool towel, splash of cold water on face and neck, going inside where there is AC, etc).
- Be particularly vigilant around the extremes of ages. Infants and young children don’t regulate their body temperature as well as adults, so they can overheat much more quickly. On the other end of the spectrum, older adults may not feel thirsty as often, or may forget to hydrate, especially if they live alone or have memory issues.
- Medications can also play a role. Common prescriptions like diuretics, beta-blockers, and certain antidepressants (SSRI’s) or antihistamines can affect hydration or interfere with the body’s ability to regulate temperature, which increases the risk of heat-related illness.
About Dr. Solomon Behar
Solomon Behar, M.D., is a pediatric emergency medicine physician at Columbia Emergency Medical Group. He is certified by the American Board of Pediatrics in general pediatrics and pediatric emergency medicine, Dr. Behar has been practicing pediatric emergency medicine in Southern California for 10 years. He/she graduated from University of Nevada School of Medicine and completed his residency and fellowship at Children’s Hospital Los Angeles.
His practice focuses on care of the acutely ill and injured child. His special interests include medical education and pediatric disaster medicine. He is the senior medical editor of the international Continuing Medical Education (CME) podcast Pediatrics Reviews and Perspectives (Peds RAP) and a regular contributor to the CME podcast Emergency Medicine Reviews and Perspectives (EM RAP).
